

To accompany the Pulmonary Perspectives® article by Drs. P. Rali, Potarazu, A. Rali, and Moores from the Summer 2026 print edition, we would like to highlight the treatment section of the 2026 American Heart Association (AHA)/American College of Cardiology (ACC) guideline for pulmonary embolism (PE).1 The guideline notably expands the recommended scope of catheter-based interventions for patients at increased risk of clinical deterioration and provides an in-depth discussion of the role of reperfusion therapies to treat PE.
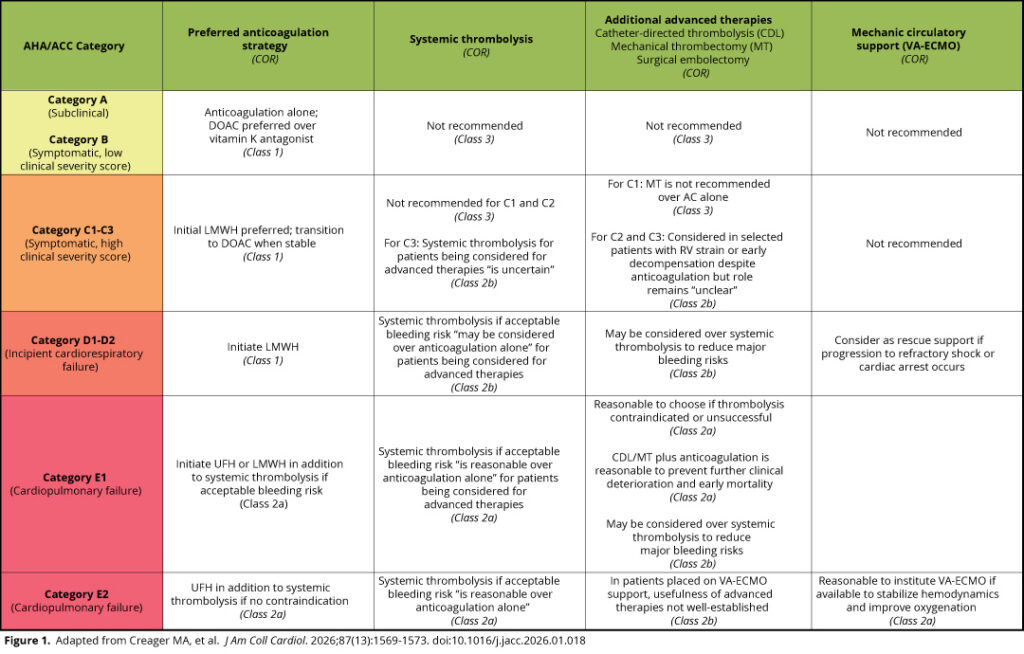
The cornerstone of PE treatment remains the timely initiation of anticoagulation. For patients in clinical categories A and B, which align with the low-risk group in the European Society of Cardiology (ESC) guidelines, the recommendation is initiation of a direct oral anticoagulant (DOAC) over vitamin K antagonist in most patients, including those with obesity, nonsevere chronic kidney disease, and brain tumors.2 For patients at higher risk of clinical deterioration (AHA/ACC Categories C, D, and E), the recommendation is to initiate treatment with low-molecular-weight heparin (LMWH) rather than unfractionated heparin (UFH).

This recommendation applies to essentially all patients, including those with impaired renal function and obesity, who may require LMWH dosing adjustments. This is based on increasing evidence that patients treated with LMWH achieve therapeutic anticoagulation levels more quickly and reliably, have fewer bleeding complications, and have a lower incidence of heparin-induced thrombocytopenia.3 While UFH can continue to be used to treat any patient with PE requiring parenteral therapy, particularly in institutions with high-quality anticoagulation protocols, the only scenario in which these new guidelines suggest UFH over LMWH is in Category E2 (refractory shock or cardiac arrest), where venoarterial extracorporeal membrane oxygenation (VA-ECMO) is a consideration.
When considering catheter-based interventions, surgical embolectomy, or systemic thrombolysis, the authors acknowledge that the choice between UFH and LMWH in these scenarios is driven primarily by small studies and expert opinion. A small, retrospective study comparing patients treated with UFH vs LMWH before catheter-directed lysis found no difference in the rate of adverse events between groups; these results are subject to selection bias due to the retrospective nature of the data.4 Though not meant to compare parenteral anticoagulation strategies, mechanical thrombectomy studies such as FLARE and PEERLESS included patients who were being treated with LMWH without an obvious safety signal favoring UFH.5–6 The conclusion is that LMWH provides superior anticoagulation coverage, and its administration should not prevent advanced therapies when indicated.

The data is even more limited when selecting an anticoagulation strategy in a patient who may require systemic thrombolytics. A single observational study comparing patients treated with UFH vs LMWH following thrombolysis for acute PE found that the LMWH group was more likely to survive to 30 days, though results were also subject to selection bias, as the study was not randomized.7 Overall, LMWH is a reasonable option for the vast majority of patients requiring parenteral anticoagulation for PE.
Most notably, the guideline places systemic thrombolysis in the same category as catheter-based thrombolysis (CDL), mechanical thrombectomy (MT), and surgical embolectomy; all are considered reperfusion therapies with varying levels of evidence. Patients in Category E2 (refractory cardiogenic shock or cardiac arrest) should still receive systemic thrombolytics over other reperfusion therapies. Interestingly, the strength of recommendation for all reperfusion options is the same for all patients in Category E1 (persistent hypotension with shock), with no single option recommended with higher confidence. It is suggested that reperfusion therapies be considered for all patients in Category D (either transient hypotension or normotensive shock); all reperfusion options are given the same strength of recommendation here as well. The strength of recommendation for reperfusion therapy separates in Category C. The role of CDL and MT remains “unclear” for patients who fall into Categories C2 or C3, whereas the use systemic thrombolysis is not recommended for patients in Categories C1 and C2 due to risk of harm.
As newer studies compare various reperfusion strategies with anticoagulation alone, including the recently published HI-PEITHO trial, we expect PE management to continue to evolve.8 Evaluating management options using this new classification system may become challenging, as enrollment criteria for these studies rely heavily on the ESC risk-stratification model. These studies enrolled the extremely heterogenous intermediate-risk patient group, so it remains to be seen exactly which patient subgroups stand to benefit the most from advanced therapies.
While this guideline expands the indication for reperfusion therapies, high-quality data is still needed to ensure that patients are not exposed to more harm than anticoagulation alone. Pulmonary embolism response teams can help navigate these evidence gaps to select timely interventions and preferred anticoagulation strategies.
References
1. Writing Committee Members, Creager MA, Barnes GD, et al. 2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN guideline for the evaluation and management of acute pulmonary embolism in adults: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2026;153(12):e977-e1051. doi:10.1161/CIR.0000000000001415
2. Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020;41(4):543-603. doi:10.1093/eurheartj/ehz405
3. Robertson L, Jones LE. Fixed dose subcutaneous low molecular weight heparins versus adjusted dose unfractionated heparin for the initial treatment of venous thromboembolism. Cochrane Database Syst Rev. 2017;2(2):CD001100. doi:10.1002/14651858.CD001100.pub4
4. Graif A, Kimbiris G, Grilli CJ, Agriantonis DJ, Putnam SG, Leung DA. Safety of therapeutic anticoagulation with low-molecular-weight heparin or unfractionated heparin infusion during catheter-directed thrombolysis for acute pulmonary embolism. J Vasc Interv Radiol. 2020;31(4):537-543. doi:10.1016/j.jvir.2019.12.003
5. Tu T, Toma C, Tapson VF, et al. A prospective, single-arm, multicenter trial of catheter-directed mechanical thrombectomy for intermediate-risk acute pulmonary embolism: the FLARE study. JACC Cardiovasc Interv. 2019;12(9):859-869. doi:10.1016/j.jcin.2018.12.022
6. Jaber WA, Gonsalves CF, Stortecky S, et al. Large-bore mechanical thrombectomy versus catheter-directed thrombolysis in the management of intermediate-risk pulmonary embolism: primary results of the PEERLESS randomized controlled trial. Circulation. 2025;151(5):260-273. doi:10.1161/CIRCULATIONAHA.124.072364
7. Senturk A, Ucar EY, Berk S, et al. Should low-molecular-weight heparin be preferred over unfractionated heparin after thrombolysis for severity pulmonary embolism? Clin Appl Thromb Hemost. 2016;22(4):395-399. doi:10.1177/1076029614564863
8. Rosenfield K, Klok FA, Piazza G, et al. Ultrasound-facilitated, catheter-directed fibrinolysis for acute pulmonary embolism. N Engl J Med. Published online March 28, 2026. doi:10.1056/NEJMoa2516567
