

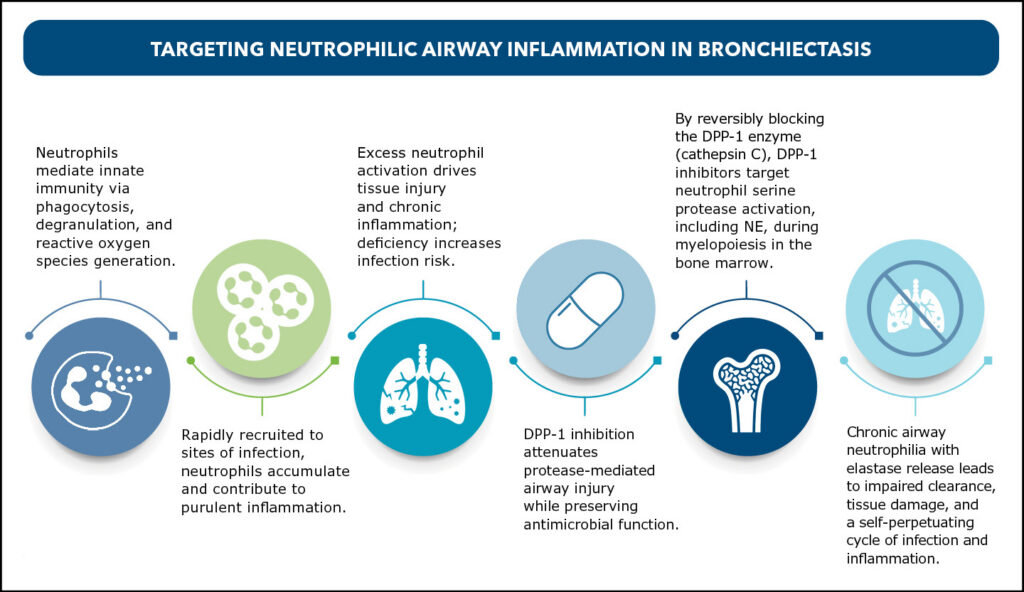
The US Food and Drug Administration’s approval of brensocatib in 2025 marked the first potential disease-modifying therapy for noncystic fibrosis (non-CF) bronchiectasis and the first approved dipeptidyl peptidase 1 (DPP-1) inhibitor.1–2 Unlike traditional symptomatic care, DPP-1 inhibition targets the underlying driver of disease: neutrophilic airway inflammation. Reversibly blocking the DPP-1 enzyme (cathepsin C) in the bone marrow impairs the activation of neutrophil serine proteases (NSPs), including neutrophil elastase (NE), while preserving other neutrophil functions. This treatment “defangs” the developing neutrophils, reducing the release of harmful proteolytic enzymes at disease sites like the lungs, thereby attenuating inflammation.3–8
In the phase 3 ASPEN and phase 2 WILLOW trials, once-daily oral brensocatib significantly reduced pulmonary exacerbations compared with placebo, with the 25 mg dose also slowing lung function decline (FEV₁) in patients 12 years or older.1,9 Although guidelines are still evolving, DPP-1 inhibitors are expected to become a new standard of care, with ongoing studies further defining their role in bronchiectasis management.
Early real-world and observational clinical experience suggests DPP-1 inhibition reduces health care use, decreases antibiotic use, improves respiratory symptoms and patient-reported outcomes, and is generally well-tolerated, though longer-term data are needed.
Although no validated biomarker currently guides therapy in bronchiectasis, clinical decision-making is supported by well-established disease characteristics. Unlike asthma or COPD, where blood eosinophils and other biomarkers inform biologic use, bronchiectasis management relies on a comprehensive clinical assessment of neutrophilic activity. In practice, treatment decisions are informed by exacerbation frequency, symptom burden, and overall clinical impact. This clinically driven approach enables individualized patient selection, with therapeutic positioning expected to further evolve as emerging evidence and biomarker development advance.
Early clinical experience with DPP-1 Inhibition
Though longer-term data are needed, early real-world and observational clinical experience suggests DPP-1 inhibition:
- Reduces health care use
- Decreases antibiotic use
- Improves respiratory symptoms and patient-reported outcomes
- Is generally well-tolerated
Although no validated biomarker currently guides therapy in bronchiectasis, clinical decision-making is supported by well-established disease characteristics.
Unlike asthma or COPD, where blood eosinophils and other biomarkers inform biologic use, bronchiectasis management relies on a comprehensive clinical assessment of neutrophilic activity. In practice, treatment decisions are informed by:
- Exacerbation frequency
- Symptom burden
- Overall clinical impact
This clinically driven approach enables individualized patient selection, with therapeutic positioning expected to further evolve as emerging evidence and biomarker development advance.
This article was originally published in the Summer 2026 issue of CHEST Physician.
References
1. Chalmers JD, Burgel PR, Daley CL, et al. Phase 3 trial of the DPP-1 inhibitor brensocatib in bronchiectasis. N Engl J Med. 2025;392(16):1569-1581. doi:10.1056/NEJMoa2411664
2. Insmed. FDA approves BRINSUPRI™ (brensocatib) as the first and only treatment for non-cystic fibrosis bronchiectasis, a serious, chronic lung disease. Published August 12, 2025. https://www.multivu.com/insmed/9347351-en-fda-approves-brinsupri-brensocatib
3. Headley D, Dowey R, Turton H, et al. Investigating the impact of dipeptidyl peptidase-1 inhibition in humans using multi-omics. J Allergy Clin Immunol. 2025;156(5):1356-1367. doi:10.1016/j.jaci.2025.07.016
4. Tang RD, Yue JQ, Chalmers JD, Guan WJ. Dipeptidyl peptidase 1 inhibitors and neutrophilic inflammation in bronchiectasis: a narrative review. J Thorac Dis. 2025;17(7):5347-5360. doi:10.21037/jtd-2025-289
5. Zhang D, Zhang W, Hu P, Zhang W. Dipeptidyl peptidase 1 inhibitors for inflammatory respiratory diseases: mechanisms, clinical trials, and therapeutic prospects. Front Pharmacol. 2025;16:1656316. doi:10.3389/fphar.2025.1656316
6. Emara A, Awashra A, Ellebedy M, et al. Efficacy and safety of DPP-1 inhibitors in bronchiectasis: a GRADE-assessed meta-analysis of randomized controlled trials. Respir Res. 2025;26(1):332. doi:10.1186/s12931-025-03407-2
7. Bell SC, Grimwood K. Brensocatib in bronchiectasis—a new sheriff in town? N Engl J Med. 202524;392(16):1647-1648. doi:10.1056/NEJMe2502618
8. Johnson E, Gilmour A, Chalmers JD. Dipeptidyl peptidase-1 inhibitors in bronchiectasis. Eur Respir Rev. 2025;34(176):240257. doi:10.1183/16000617.0257-2024
9. Cipolla D, Zhang J, Korkmaz B, et al. Dipeptidyl peptidase-1 inhibition with brensocatib reduces the activity of all major neutrophil serine proteases in patients with bronchiectasis: results from the WILLOW trial. Respir Res. 2023;24(1):133. doi:10.1186/s12931-023-02444-z
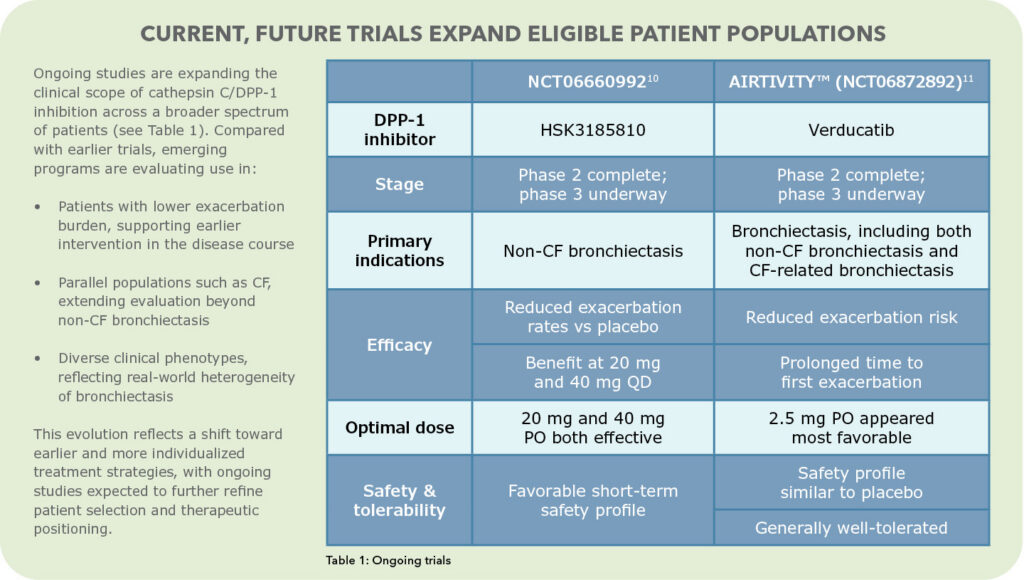
10. Zhong NS, Qiu R, Cao J, et al; SAVE-BE trial investigators. Effects of the DPP-1 inhibitor HSK31858 in adults with bronchiectasis in China (SAVE-BE): a phase 2, multicenter, double-blind, randomized, placebo-controlled trial. Lancet Respir Med. 2025;13(5):414-424. doi:10.1016/S2213-2600(25)00019-0
11. Chalmers JD, Shteinberg M, Mall MA, et al. Cathepsin C (dipeptidyl peptidase 1) inhibition in adults with bronchiectasis: AIRLEAF, a phase II randomized, double-blind, placebo-controlled, dose-finding study. Eur Respir J. 2025;65(1):2401551. doi:10.1183/13993003.01551-2024