

The latest guidelines from the American Heart Association (AHA) and American College of Cardiology focus on the evaluation and management of acute pulmonary embolism (PE) in adults. They come nearly a decade after the previous set of AHA guidelines. The current guidelines are endorsed by nine other societies, including CHEST, which had representatives on the writing panel and peer review group.1 These guidelines are being published at the dawn of several randomized controlled trials in acute PE, albeit only one (the PEERLESS trial) was published prior to the release of the guidelines.2 Others, including Hi-PEITHO, STORM-PE, PEITHO-3, and PEERLESS 2, are ongoing or were published afterward.2–6
The AHA guidelines focus on diagnosis, risk stratification, and management of acute PE. Unlike the 2021 CHEST guidelines, they do not address deep vein thrombosis (DVT) or the prevention and recurrence of VTE.7
A key feature of the AHA guidelines is the panel’s proposed new classification of acute PE severity. This classification parallels the Society of Cardiovascular Angiography and Interventions’ (SCAI) stages for cardiogenic shock (CS), which in recent years have found wide acceptance. The SCAI system divides CS into stages A through E: A (at risk), B (beginning), C (classic), D (deteriorating), and E (extremis).
Our review focuses primarily on this proposed classification and its ability to risk-stratify patients. The specifics of proposed treatment algorithms will be deferred to a subsequent review.
Introduction of new PE classification
The current classification most widely used and endorsed is that proposed by the European Society of Cardiology (ESC), which classifies PE into low, intermediate-low, intermediate-high, and high-risk categories. These categories are based on expected short-term (30-day) mortality. Intermediate-risk PE encompasses a very heterogeneous group, as patients may present anywhere on the spectrum of clinically stable to nearing hemodynamic collapse.
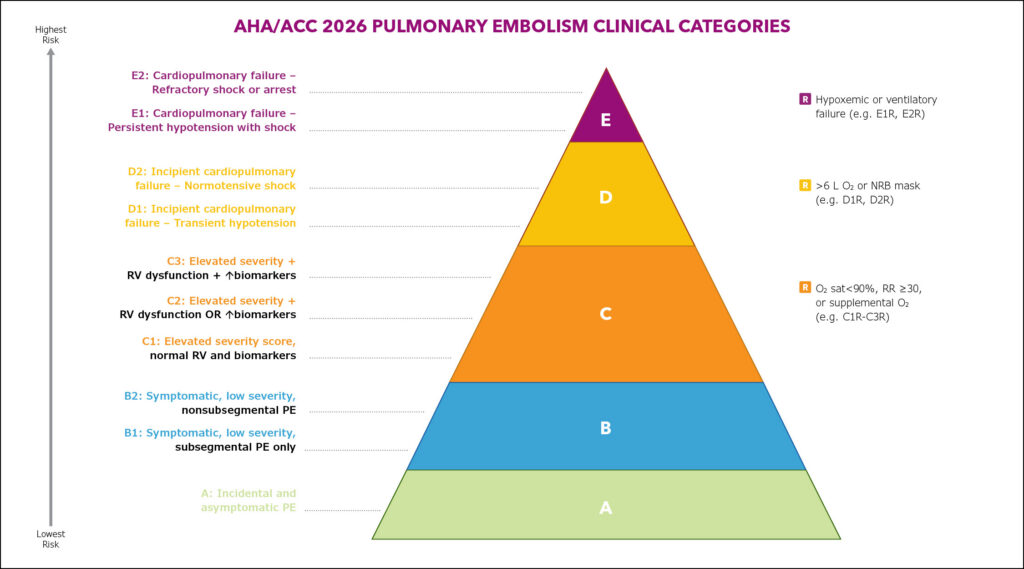
The new AHA classification adopts the SCAI framework, grouping patients into Categories A through E with respiratory modifiers. Unlike prior systems, this model incorporates respiratory decompensation specifically in Categories C through E. Notably, SCAI Stage C represents classic CS, while in this new classification for PE, Category E represents classic obstructive shock. The hope is that this new framework will better define the dynamic spectrum between intermediate and high-risk PE.
Category A includes incidental PE. Categories B1 and B2 include patients with a low clinical severity score (such as the Pulmonary Embolism Severity Index [PESI] or its simplified version [sPESI]) presenting with either subsegmental or nonsubsegmental PE. These patients would have been considered low-risk PE in the ESC classification. Category B highlights that some patients with symptoms may have proximal clots but lack abnormal risk scores or biomarkers, requiring only anticoagulation.

Category C has three subcategories. Patients in Category C1 present with an elevated severity score but normal right ventricular (RV) function and cardiac biomarkers, such as troponin or brain natriuretic peptides (BNP). The presence of either RV dysfunction on imaging or abnormal biomarkers leads to a C2 categorization. Patients in Category C3 have both RV dysfunction and abnormal biomarkers. The inclusion of BNP alongside troponin is a new feature of the updated guidelines, although the ESC guidelines do note that an elevated BNP may provide additional prognostic information. Respiratory modifiers are to be applied in Categories C1 through C3 if oxygen saturation drops below 90%, respiratory rate is high, or supplemental oxygen is required.
Category D introduces a new hemodynamic category of incipient cardiopulmonary failure. Patients in Category D1 experience transient hypotension, while patients in Category D2 have evidence of systemic hypoperfusion (elevated lactate, acute kidney injury, low urine output, or elevated Composite Pulmonary Embolism Shock [CPES] score). The inclusion of transient hypotension as a preshock stage (D1) is a new addition. D2 builds on the concept of normotensive shock. In Category D, respiratory modifiers include high oxygen needs (> 6 L/min) or escalation to nonrebreather mask.
Category E represents true obstructive shock. Stage E1 includes those with recurrent or persistent hypotension (classic high-risk PE). Stage E2 represents catastrophic PE, characterized by refractory cardiogenic shock or cardiac arrest due to PE. Category E also includes a respiratory modifier for patients requiring ventilatory support. Figure 1 illustrates the acute PE clinical categories, emphasizing the continuum of physiologic severity captured by the new classification.
New parameters in this classification
The 2026 AHA classification incorporates additional risk scores and physiologic markers—including the CPES score, National Early Warning Score 2 (NEWS2), serum lactate, and recognition of normotensive shock—reflecting a shift toward earlier identification of decompensation in acute PE. Recognition of normotensive shock addresses a key limitation of prior classifications by identifying patients with preserved systemic BP but impaired perfusion.
The CPES score was derived from the FlowTriever All-Comer Registry for Patient Safety and Hemodynamics registry to identify normotensive patients with acute PE and low cardiac index.8 It incorporates markers of RV dysfunction (imaging and biomarkers), ischemia, central clot burden, risk of further embolization (eg, concomitant DVT), and cardiovascular compensation (eg, tachycardia). The score was subsequently validated in an independent cohort of normotensive patients with acute symptomatic PE from the PROTECT study.9 Alongside the CPES score, the Bova, PESI, and sPESI scores have been validated in hemodynamically stable patients to identify those at higher risk of adverse outcomes; however, no single score demonstrates clear superiority, and clinicians are encouraged to apply judgment when selecting among tools.1,10–11
Similarly, NEWS2, a generic early-warning system based on dynamic vital sign assessment, has shown performance comparable to PE-specific scores with the added advantage of enabling serial assessment.1 The recently published Hi-PEITHO trial underscores the relevance of physiologic risk markers such as NEWS2, demonstrating that ultrasound-facilitated catheter-directed thrombolysis plus anticoagulation reduced the composite outcome vs anticoagulation alone. This was primarily driven by reductions in hemodynamic collapse, with analysis suggesting a key contribution of NEWS2-defined risk.3 Serum lactate further refines risk assessment, with elevated levels associated with a 4.54-fold increase in all-cause mortality in normotensive PE.12
Reflections and directions: A balanced perspective
The new classification system represents a sophisticated shift toward a more granular understanding of acute PE, moving beyond binary risk models into a spectrum of physiological decompensation. By integrating markers like serum lactate, CPES score, and the recognition of normotensive shock, this framework offers the promise of identifying patients who may benefit from closer monitoring and early interventions to restore perfusion before overt collapse occurs. It elegantly bridges the gap between intermediate and high-risk categories by using a language of shock stages (the A through E framework) already familiar to many pulmonary and cardiovascular clinicians.
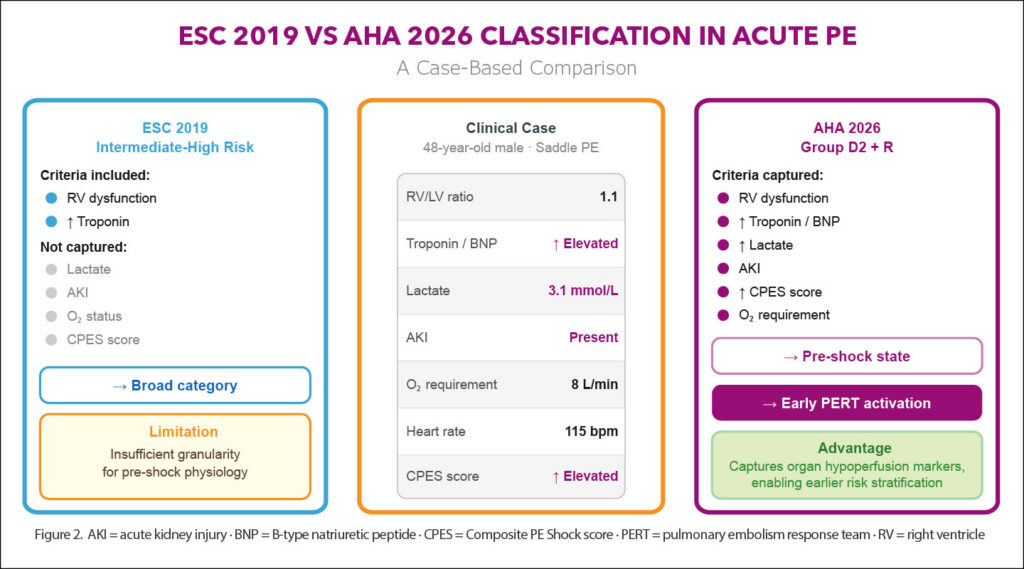
Figure 2 demonstrates a representative case that highlights the added granularity of the AHA classification compared with the previous ESC framework. However, a note of caution is warranted. While this system is rooted in published literature regarding prognostic markers, the classification itself remains largely expert opinion-based. Unlike the ESC classification, which has undergone extensive validation, this new AHA model has yet to be tested for its real-world predictive accuracy. Furthermore, while the guidelines tie specific treatment recommendations to these proposed categories, such a leap may be premature until the framework is rigorously vetted.
Moving forward
To move this classification from a conceptual framework to a clinical standard, several steps are essential. Retrospective validation utilizing large-scale databases and existing registries (such as the Pulmonary Embolism Response Team or Registro Informatizado de Enfermedad TromboEmbólica) to determine if these specific categories accurately predict clinical outcomes would be the first step.
Next, investigators should incorporate the A through E stages into the design of future management trials to see whether category-specific interventions truly improve survival or reduce morbidity. Conducting well-designed meta-analyses to harmonize the data emerging from recently published and ongoing randomized controlled trials soon to be completed may also increase our understanding.
Ultimately, while the 2026 AHA guidelines provide a much-needed physiological road map for the modern PE specialist, clinicians must continue to apply sound bedside judgment while the evidence base catches up to expert consensus.
This article was originally published in the Summer 2026 issue of CHEST Physician.
References
1. Writing Committee Members, Creager MA, Barnes GD, et al. 2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN guideline for the evaluation and management of acute pulmonary embolism in adults: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2026;153(12):e977-e1051. doi:10.1161/CIR.0000000000001415
2. Jaber WA, Gonsalves CF, Stortecky S, et al. Large-bore mechanical thrombectomy versus catheter-directed thrombolysis in the management of intermediate-risk pulmonary embolism: primary results of the PEERLESS randomized controlled trial. Circulation. 2025;151(5):260-273. doi:10.1161/CIRCULATIONAHA.124.072364
3. Rosenfield K, Klok FA, Piazza G, et al. Ultrasound-facilitated, catheter-directed fibrinolysis for acute pulmonary embolism. N Engl J Med. Published online March 28, 2026. doi:10.1056/NEJMoa2516567
4. Lookstein RA, Konstantinides SV, Weinberg I, et al. Randomized controlled trial of mechanical thrombectomy with anticoagulation versus anticoagulation alone for acute intermediate-high risk pulmonary embolism: primary outcomes from the STORM-PE trial. Circulation. 2026;153(1):21-34. doi:10.1161/CIRCULATIONAHA.125.077232
5. A reduced dose of thrombolytic treatment for patients with intermediate high-risk acute pulmonary embolism: a randomized controled trial (PEITHO-3). ClinicalTrials.gov. https://clinicaltrials.gov/study/NCT04430569
6. PEERLESS II: RCT of FlowTriever vs. anticoagulation alone in pulmonary embolism. ClinicalTrials.gov. https://clinicaltrials.gov/study/NCT06055920
7. Stevens SM, Woller SC, Kreuziger LB, et al. Antithrombotic therapy for VTE disease: second update of the CHEST guideline and expert panel report. Chest. 2021;160(6):e545-e608. doi:10.1016/j.chest.2021.07.055
8. Bangalore S, Horowitz JM, Beam D, et al. Prevalence and predictors of cardiogenic shock in intermediate-risk pulmonary embolism: insights from the FLASH registry. JACC Cardiovasc Interv. 2023;16(8):958-972. doi:10.1016/j.jcin.2023.02.004
9. Najarro M, Briceño W, Rodríguez C, et al. Shock score for prediction of clinical outcomes among stable patients with acute symptomatic pulmonary embolism. Thromb Res. 2024;233:18-24. doi:10.1016/j.thromres.2023.11.011
10. Leupp S, Sarzilla S, Caruzzo CA, Landi A, Valgimigli M, Milzi A. Refining risk stratification in acute pulmonary embolism: a comparative validation of six prognostic scores in a real-life cohort. Int J Cardiol. 2026;451:134247. doi:10.1016/j.ijcard.2026.134247
11. Zhang RS, Yuriditsky E, Zhang P, et al. Choosing the right tool: comparing risk stratification models in intermediate-risk pulmonary embolism. Catheter Cardiovasc Interv. 2025;106(3):1928-1936. doi:10.1002/ccd.70016
12. Wang Y, Feng Y, Yang X, Mao H. Prognostic role of elevated lactate in acute pulmonary embolism: a systematic review and meta-analysis. Phlebology. 2022;37(5):338-347. doi:10.1177/02683555221081818